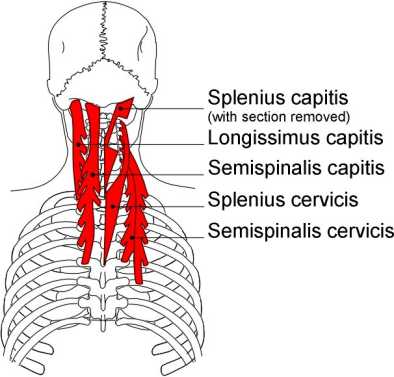
Posterior cervical muscles
Anatomy
Splenius capitis arises on the ligamentum nuchae and spinous processes of C7 to T3 and attaches under the lateral part of the superior nuchal line of the occiput and on the mastoid process of the temporal bone.
Splenius cervicis arises on the spinous processes of T3 to T6 and attach on the posterior tubercles of the transverse process C1 to T3.
Splenius capitis and splenius cervicis lie deep to sternocleidomastoid, trapezius and the rhomboids and superficial to the segmental muscles, interspinales, intertransversarii and transversospinalis.
Nerve supply: Cervical spinal nerves.
Actions:Splenius capitis and splenius cervicis contracting bilaterally extend the head and neck, contracting unilaterally they sidebend and slightly ipsilaterally rotate the head and neck.
Erector spinae
Iliocostalis cervicis arises on the superior border of the angles of ribs 3 to 6 medial to iliocostalis thoracis attachments. It attaches on the posterior tubercles of the transverse process of C4 to C6.
Longissimus cervicis arises on the transverse processes of T1 to T5 medial to longissimus thoracis and to the posterior tubercles of the transverse processes of C2 to C6.
Spinalis cervicis arises on the spinous processes of C7 to T2 and the ligamentum nuchae. It attaches on the spinous processes of C2 to C4. It exhibits variation in its attachments and may be absent.
Cervical spinous processes may be bifid. C2 and C7 (vertebra prominens) are easily palpable. C6 is usually palpable but disappears in extension. Articular pillars and facet joints are at finger width spacings.
Transversospinalis
Semispinalis thoracis arises on the transverse processes of T6 to T10 and attaches on the spinous processes of C6 to T4. More tendon in form.
Semispinalis cervicis arises on the transverse processes of T1 to T6 and attaches on the spinous processes of C2 to C5. More muscular especially the fibres that attach on the axis.
Semispinalis capitis arises on the transverse processes of C7 to T6 and the articular processes of C4 to C6 (sometimes C7 & T1) and attaches either side of the mid-sagittal line between the superior and inferior nuchal lines on the occiput.
Nerve supply: Dorsal rami of cervical and thoracic nerves.
Action: Extension of the head and cervical spine.
Multifidus arise on the sacrum (S4), aponeurosis of the erector spinae, posterior superior iliac spine, posterior sacro-iliac ligament, mamillary processes of L1 to L5, transverse processes of T1 to T12 and articular processes of C4 to C7. The muscle attaches along the length of a spinous process one to four vetebral segments above.
Nerve supply: Dorsal rami of the spinal nerves.
Rotatores are the deepest muscles. They arise on cervical, thoracic and lumbar transverse processes and attach on the lamina and base of the spinous process of the vertebra above. Nerve supply: Dorsal rami of the spinal nerves.
Interspinales run from one spinous process to the spinous process above. They are present between C2 and T3, and between T11 and L5. They are more distinct in the cervical spine. Sometimes they occur between L5 and the sacrum.
Nerve supply:Dorsal rami of the spinal nerves.
Intertransversarii run from a transverse process to the transverse process above. They are present between C1 and T1, and between T10 and the sacrum. In the cervical and lumbar, pairs of muscles lie either side of the spine.
Nerve supply: Dorsal and ventral rami of the spinal nerves.
Technique 3 Inhibition or posterior cervical muscles from C2 to C6
Patient
- Prone with head rotated away from the therapist.
Therapist
- Stand by the side of the couch near to the patient's head.
- For greatest control grasp a broad area of the crown of the patients head in your cephalad hand (optional)
- Grasp the patients neck gently with your caudad hand and place the tip of your thumb on a posterior cervical muscle and articular pillar on the side of the spine nearest the table.
Applicator
- The tip of the thumb of your caudad hand.
Tissue tension
- Take up the primary tissue tension by increasing your thumb pressure on the muscle.
- Take up the secondary tissue tension with a small amount of thumb rotation.
- Take up the longitudinal tissue tension by slightly flexing the patient's neck.
- To prevent over-tension of the superficial muscles and fascia keep the head in slight extension.
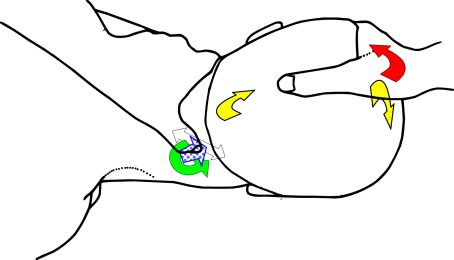 Figure 4.5
Figure 4.5| Muscle Fibres | Primary Force | Secondary Force | Stretch Force | Contraction Force |
Active component
- Ask the patient to take in a deep breath and hold it.
- Ask the patient to push their neck straight backwards into your applicator (neck extension) for 3 to 5 seconds.
- Alternatively ask the patient to rotate their head into the table.
- A light pressure is all that is needed, about 10% of maximum contraction.
- Resist their effort with your applicator, not with your cephalad hand.
- Ask the patient to relax and then take up the tissue slack presented by increasing your thumb pressure and re-positioning the patient's cervical spine in greater flexion.
- Repeat several times or as required.
Technique 4 Unilateral kneading of posterior cervical muscles from the occiput to C7.
Patient
- Supine with head straight and resting on a folded towel or shallow pillow.
Therapist
- Stand at the side of the table opposite the patient's head.
- Grasp and support the patient's head with a broad hold over the frontal bone with your cephalad hand.
- Reach across the patient with your caudad hand and hook your fingertips around the opposite side posterior cervical muscles.
- Your fingertips sit in the depression in the middle of the back of neck.
- The pads of your fingertips rest against the medial side of the posterior cervical muscles.
Applicator
- The fingertips of your caudad hand.
Tissue tension
- Take up the primary tissue tension with compression by increasing your fingertip pressure and add a transverse force to the muscle by flexing your fingertips.
- Alternatively keep your fingertips in a fixed flexed position and your forearm extended and lean back.
- Pull the muscle away from the spine.
- Work perpendicular to the muscle, from medial to lateral.
- Longitudinal tension is taken up by starting the technique with the spine in slight flexion.
- Try to maintain some flexion for the duration of the technique. A pillow may be placed under the patient's head to prevent hyperextension of the head and neck.
- Further tension is taken up by rotating the patient's head away from you.
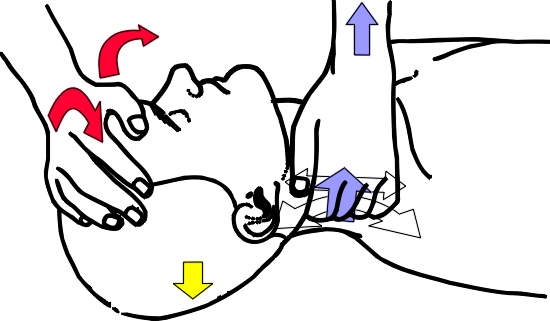 Figure 4.6
Figure 4.6| Muscle Fibres | Primary Force | Secondary Force | Stretch Force | Contraction Force |
Kneading
- With the fingertips of your caudad hand apply a rhythmical cycle of primary, secondary and longitudinal forces.
- When the muscle is at an optimal longitudinal tension increase the primary forces.
- Use a push-pull action.
- Keep your wrist and the palm of your caudad hand away from the patient's neck. Do not allow your hand to obstruct movement of the cervical spine or reduce the force going through to your fingertips (the applicator).
- Your pressure should be just short of discomfort.
- To relax the muscle, work with the patients breathing cycle, about 15 breaths per minute.
- To stimulate increase your speed to about 40 cycles per minute.
 Picture 4.4
Picture 4.4Active component
- Ask the patient to take in a deep breath and hold it.
- Ask the patient to contract their posterior cervical muscles by pushing their head backward into the table for 3 to 5 seconds using a 10% effort.
- Alternatively ask the patient to rotate their head into your applicator.
- Resist the patient's effort and maintain tissue lockup throughout the technique.
- Ask the patient to exhale and to relax their muscle contraction.
- As soon as you feel that the patient has relaxed their muscles completely (about 1-3 seconds) take up the tissue slack by increasing the primary tension, secondary and longitudinal tension.
- Take up the slack after each contraction and during exhalation.
- Repeat 2 or 3 times or as required.