30. Lateral forearm (extensor) muscles
Anatomy
|
Brachioradialis is the most lateral muscle. It arises on the lateral supracondylar ridge and attaches on the lateral side of radial styloid process. It is more easily observed with resisted elbow flexion half way between pronation and supination.
Extensor carpi ulnaris is the most medial of the extensor muscles. It arises on the lateral epicondyle and posterior ulna and attaches on to the base of the 5th metacarpal.
Extensor carpi radialis longus arises on the lateral supracondylar ridge of humerus and attaches on the posterior base of the 2nd metacarpal.
Extensor carpi radialis brevis arises on the lateral epicondyle of humerus and attaches on the posterior base of the 3rd metacarpal.
|
 |
Extensor digitorum communis arises on the lateral epicondyle of the humerus and attaches on the base of the 2nd and 3rd phalanges of all 4 fingers.
Action: extension of hand and fingers.
Nerve supply to extensors: Radial nerve.
Supinator forms the lateral floor of the cubital fossa. It arises on the lateral epicondyle of humerus and ulna below the radial notch, and winds around the radius anteriorly to insert on the lateral surface of the radius and radial tubercle.
Action: supination of the forearm, wrist and hand.
Technique 1 Kneading of all muscles listed above.
Patient
- Supine with the arm resting on the table by the side of the body.
Therapist
- Stand at the side of the table level with the patient's abdomen.
- Grasp the patient's hand with your caudad or cephalad hand and flex their wrist.
- Abduct their arm to about 30 degrees and flex their forearm to 90 degrees.
- Reach around the patient's forearm with your other hand and hook your fingertips around the muscle you are treating.
- Your thumb rests as an anchor on the posterior border of patient's ulna to enable the fingers to grip the appropriate muscle fibres firmly.
Applicator
- The fingertips of your cephalad hand work across the muscle in a lateral direction.
- Alternatively work the fingertips of your caudad hand in a medial direction.
- You fingertips should be together.
Tissue tension
- Keep your wrist anchored to the patient's ulna.
- Take up the primary tissue tension with compression and a transverse force achieved by flexing your fingertips.
- Your force is perpendicular to the muscle.
- Longitudinal tension is taken up by flexing the patient's wrist.
- Secondary tension is taken up by rotating the patient's forearm in the opposite direction to your primary force. Supinate when using your caudad hand as the applicator and pronate when using your cephalad hand as the applicator.
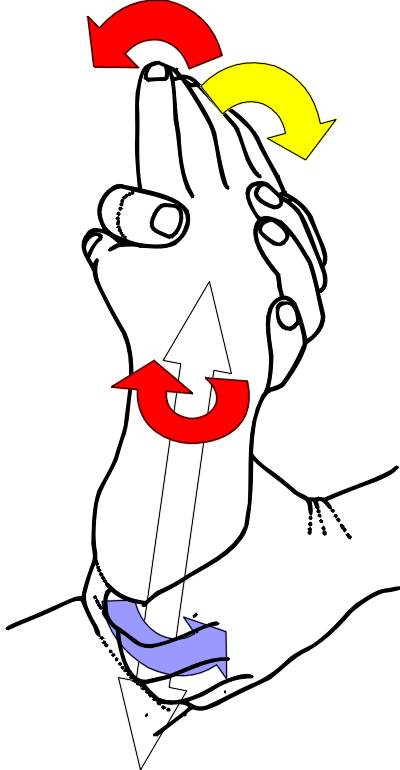 Figure 30.1
Figure 30.1| Muscle Fibres | Primary Force | Secondary Force | Stretch Force | Contraction Force |
Kneading
- With the fingertips of one hand apply a rhythmical cycle of primary, secondary and longitudinal forces.
- Your hooked fingertips pull back on the muscle as you pronate or supinate and flex the wrist.
- When the muscle is at an optimum longitudinal and secondary tension increase the primary force.
- Your pressure should be just short of discomfort.
- Start at the proximal attachment of the muscle and work your way down the forearm.
- To relax the muscle, work with the patients breathing cycle, about 15 breaths per minute.
- To stimulate increase your speed to about 40 cycles per minute.
Active component
- For the wrist and finger extensor muscles ask the patient to straighten (extend) their wrist.
- For brachioradialis ask the patient to flex their forearm.
- For supinator ask the patient to rotate (supinate) their forearm outwards.
- Contract the muscles for 3 to 5 seconds using a 10% effort.
- Resist the patient's effort and maintain tissue lockup throughout the technique.
- Ask the patient to exhale and to relax their muscle contraction.
- When you feel that the patient has relaxed their muscles completely (about 1-3 seconds) take up the tissue slack by increasing the primary, secondary and longitudinal tension.
- Take up the slack after each contraction and during exhalation.
- Repeat 2 or 3 times or as required.